Case of the Month ...
Case History
This is an FNA from the thyroid of a 34 year old woman who was diagnosed with hyperthyroidism in August 2001. Her serum TSH was <0.01 uU/ml (normal 0.50-5.00 uU/ml) and her total T3 was 272 ng/dl (normal60-181 ng/dl). The patient was treated with atenolol and subsequently with propylthiouracil. Her thyroid gland was firmly enlarged with a 1.5 cm palpable nodule in the right lobe. The nodule was sampled with the aid of ultrasound guidance.
Diagnosis & Discussion
click on image for larger version
Microscopic description:
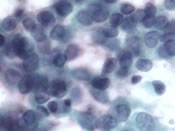
Cyto 1 and 2- follicular cells with moderate to abundant dense cytoplasm are present in a background of chronic inflammation; some of the follicular cells have pale nuclei with nuclear grooves.
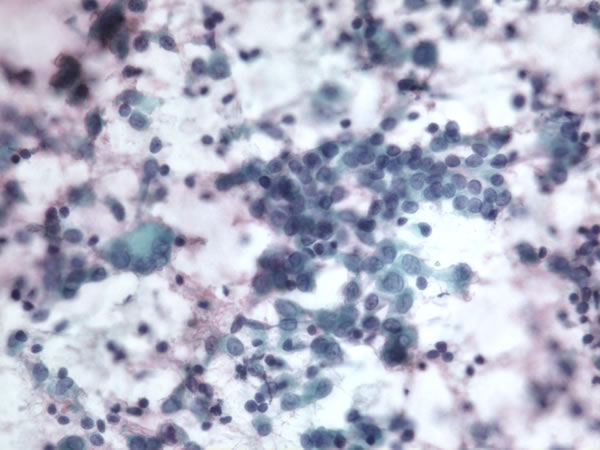
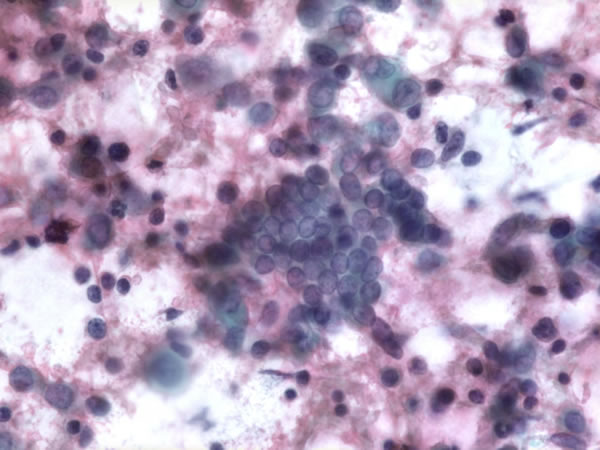
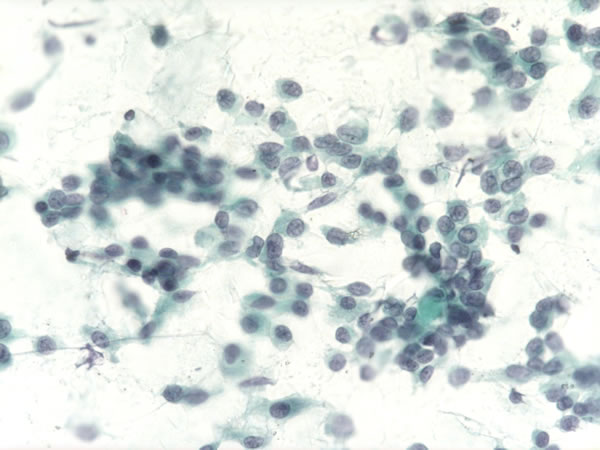
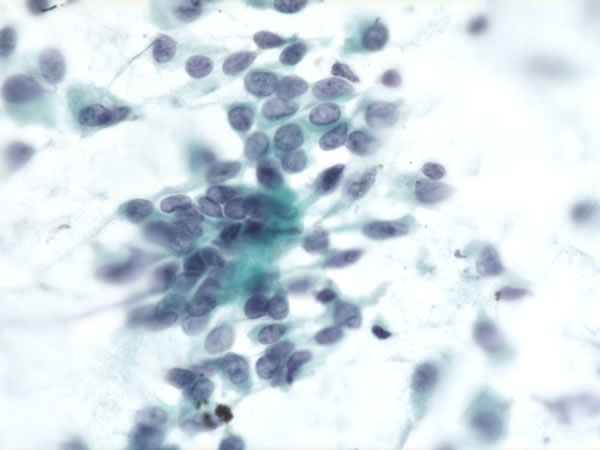
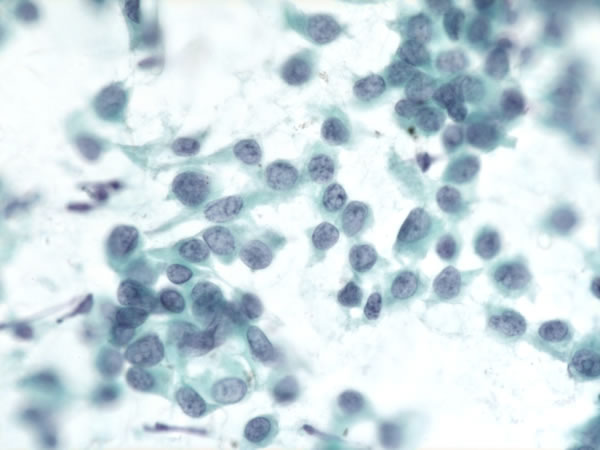
Cyto 3,4,5- Images – Atypical follicular cells are present singly and in loosely cohesive groups. The cells have a moderate amount of cytoplasm, the nuclei have fine chromatin with irregular nuclear outlines, irregular grooves and inapparent to small nucleoli. Rare possible intranuclear inclusions are identified. Some cells have a plasmacytoid appearance. No colloid or inflammation is present in the background but a rare focus of dense extracellular material is identified.
FNA diagnosis:
- Neoplastic cells present, the differential diagnosis includes papillary carcinoma and medullary carcinoma.
- Chronic thyroiditis
- Prior to surgery the serum calcitonin was found to be negative.
- Histologic diagnosis:
- Total thyroidectomy:
- Papillary carcinoma, intrathyroidal (1.4cm)
- Chronic lymphocytic thyroiditis
Histologic findings:
- Surgical 1 - The tumor is composed of masses of epithelial cells with oxyphilic cytoplasm and irregular, pale nuclei with grooves.
- Surgical 2 – Only focal papillae are present in the tumor.
- Surgical 3 – The uninvolved thyroid shows germinal centers consistent with chronic thyroiditis and follicules with evidence of colloid resorption but well developed papillae as seen in hyperthyroidism are not identified.
Discussion:
Although the nuclear morphology of the tumor cells on cytology in this case have many features suggestive of papillary carcinoma, their frequent presence as single cells, an uncommon finding in papillary carcinoma, and their occasional plasmacytoid appearance, as well as the scattered fragments of extracellular material raised the possibility of medullary carcinoma. A cellblock was not available on which to perform immunohistochemical staining for thyroglobulin and calcitonin. However, medullary carcinomas are invariably associated with elevated serum calcitonin that can be easily measured.
Little evidence of hyperthyroidism was present other than the chronic inflammation since the patient had been under treatment for several months prior to sampling. Flame cells, cytoplasmic aggregates of mauve material, can be seen on Romanowsky stained smears in cases of Grave’s disease, but we only had Papanicolaou stained material. Lymphocytes are commonly found on aspirates of the thyroid in hyperthyroidism and suggest a relationship with Hashimoto’s thyroiditis.
The incidence of hyperthyroidism (Grave's disease) in papillary carcinoma is 4 percent. Papillary carcinoma arises more commonly in lymphocytic/Hashimoto's thyroiditis