Case of the Month ...
Case History
The patient is a 82-year-old male presented with hematuria. Cystoscopy revealed an ulcerated lesion in the bladder trigone. A bladder washing was performed. (Figure 1- 4)
Diagnosis & Discussion
click on image for larger version
Figure 7
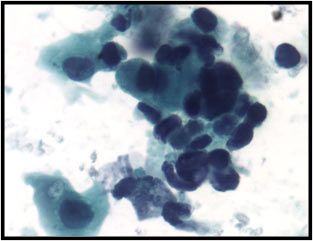
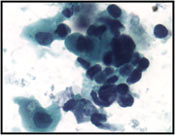
Figure 1 . Bladder washing, Pap stain. Single and clusters of small blue cells with scanty cytoplasm. The nuclear molding is present. The chromatin is dark with irregular nuclear contour and marked pleomorphism consistent with a small cell carcinoma. In addition, there are few atypical cells with moderate amount of cytoplasm and features of a urothelial carcinoma.
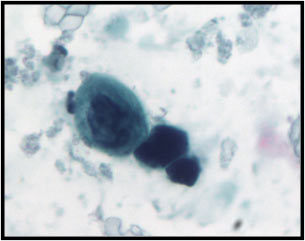
Figure 2. Bladder washing, Pap stain. Two small blue cells with irregular nuclear contour and hyperchromatic. One larger cell is also noted.
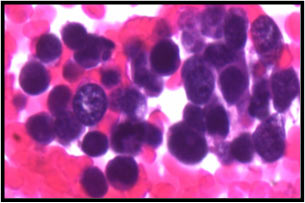
Figure 3 . Bladder washing, cell block, H&E. The small neoplastic cells are twice the size of the RBCs with finely granular chromatin and nuclear molding.
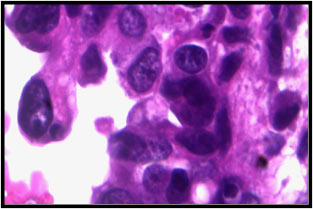
Figure 4 . Bladder washing, cell block, H&E. The larger atypical cells with moderate amount of cytoplasm and nucleoli.
Cytologic diagnosis : Small cell malignant neoplasm with features of a mixed small cell carcinoma and high-grade urothelial carcinoma. The diagnosis is supported by the result of the immunocytochemistry. (Figure 5 and 6)
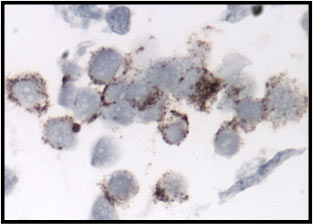
Figure 5 . Bladder washing, cell block, synaptophysin immunostain of small cell carcinoma. The tumor cells demonstrated cytoplasmic positivity.
Figure 6 . Bladder washing, cel block, pan cytokeratin immunostain. The small cell carcinoma cells showed dot-like positivity with exception of one large cell (on the left side of the field) which showed diffuse positivity.
Follow up: The patient underwent bladder biopsy and resection subsequently. A 3.5 cm trigone tumor was resected. The histology sections demonstrated mixed poorly differentiated urothelial carcinoma and small cell carcinoma (Figures 7-9). Immunohistochemical stains were performed and the tumor cells are positive for CK7, CK20, synaptophysin (Figure 10, small cell carcinoma component), and chromogranin. A subsequent radical cystectomy revealed a remainder tumor of 4.5 cm with multiple positive lymph nodes.
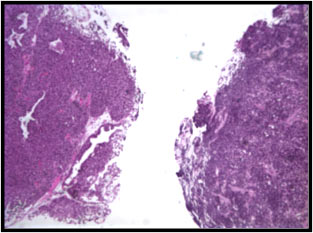
Figure 7 . Excisional biopsy of bladder trigone tumor, H&E. The tissue fragment on the left demonstrated a urothelial carcinoma. The tissue fragment on the right showed a small cell carcinoma.
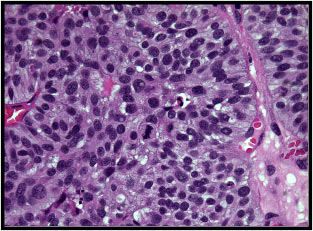
Figure 8 . Excisional biopsy of bladder trigone tumor, H&E. Urothelial carcinoma with active mitotic activity.
Figure 9 . Excisional biopsy of bladder trigone tumor, H&E. Small cell carcinoma.
Figure 10 . Excisional biopsy of bladder trigone tumor, synaptophysin immunostain. The bottom half of the section is the small cell carcinoma component of the bladder tumor which demonstrated synaptophysin positivity. However, the top half of the section is urothelial carcinoma which is negative for synaptophysin.
Histologic Diagnosis: High grade urothelial carcinoma with a small cell carcinoma component.
Discussion: Neuroendocrine carcinoma consists of carcinoid tumors, large cell neuroendocrine carcinomas, and small cell carcinoma. Primary neuroendocrine carcinomas of the urinary bladder are rare. They usually involve male patients and coexist with a urothelial carcinoma 1. Among neuroendocrine tumor of the urinary bladder, small cell carcinomas are most common with more than 100 cases have been described 2-4; carcinoid tumors are much less common; and large cell neuroendocrine carcinomas are very rare with 3 cases have be reported 5.
Here we present a case of primary small cell carcinoma of the urinary bladder with mixed poorly differentiated urothelial carcinoma. The cytomorphological pattern of the bladder washing is that of a small blue cell neoplasm. The differential diagnoses include a high grade urothelial carcinoma, a small cell carcinoma of the urinary bladder, a lymphoma, as well as metastatic lesions, especially from the lung. In conjunction with the patient’s clinical presentation and clinical work-up, the cytomorphology and immunocytochemical features support the diagnosis of a primary small cell carcinoma of the urinary bladder. Subsequent surgical excision revealed a mixed poorly differentiated urothelial carcinoma and small cell carcinoma.
Making the diagnosis of a small cell carcinoma of the urinary bladder on a cytology specimen is important. Primary neuroendocrine carcinomas of the bladder usually are at advanced stage at presentation. Like in this case, the patients already have lymph node metastases at diagnosis. Although an aggressive tumor, the prognosis is better than those patients with neuroendocrine carcinoma of other sites 6. The treatment of a mixed neuroendocrine tumor with poorly differentiated urothelial carcinoma is the same as treating a pure primary neuroendocrine carcinoma of the urinary bladder.
Acknowledgement: This case is submitted by Drs. Marilyn M. Bui and Walid Khalbuss from the Department of Pathology, University of Florida Health Science Center, Jacksonville , FL
References
- Abenoza P, Manivel C, and Siblry R. Adenocarcinoma with neuroendocrine differentiation of the urinaryl bladder. Arch Pathol Lab Med 110:1062-1066, 1986
- Mills S, Wolfe J, Weiss M, et al. Small cell undifferentialted carcinoma of the urinary bladder: a light-microscopic, immunochemical, and ultrastructureal study of 12 cases. Am J Surg Pathol 11:606-617
- Grignon D, Ro J, Ayala A, et al. Small cell carcinoma of the urinary bladder: a clinicopathologic analysis of 22 cases. Cancer 69:527-536, 1992
- Ali S, Reuter V, and Zakowski M. Small cell neuroendocrine carcinoma of the urinary bladder: a clinicopathologic study with emphasis on cytologic features. Cancer 79:356-361, 1997
- Evans AJ, Al-Maghrabi J, Tsihlias J, Lajoie G, Sweet JM, and Chapman WI. Primary large cell neuroendocrine carcinoma of the urinary bladder. Arch J Pathol Lab Med 126(10): 1229-1232, 2002
- Holmang S, Borghede G, Johansson SL. Primary small cell carcinoma of the bladder: a report of 25 cases. J Urol 153:1820-1822, 1995