Case of the Month ...
Case History
The patient is a 33 year-old female who presented with right lower quadrant abdominal pain of several weeks duration. A CT scan of the abdomen showed a 5.0 x 5.0 cm irregular soft tissue right lower quadrant mass. A CT-guided fine needle aspiration was performed (figures 1 through 4).
Diagnosis & Discussion
click on image for larger version
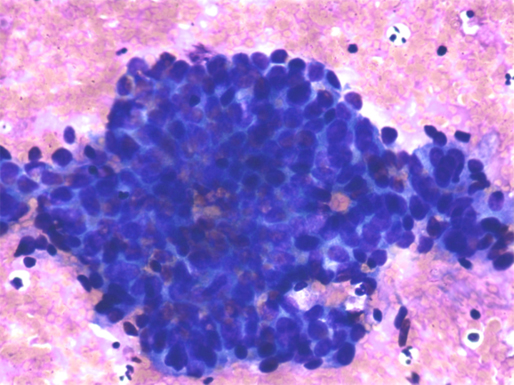
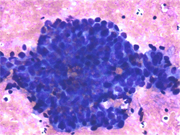
Figure 1
Diff-Quik stained slide showing cohesive group of epithelial appearing cells with scant cytoplasm Cytologic Findings:
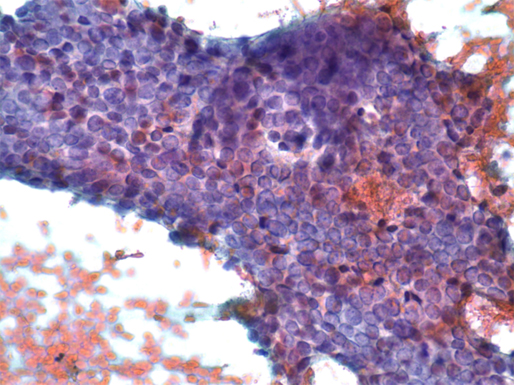
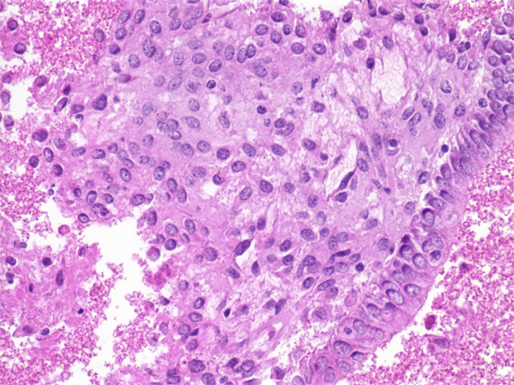
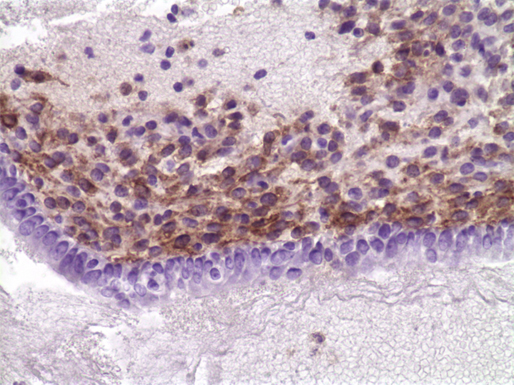
- low cuboidal to columnar glandular component with minimal nuclear atypia.
- spindled to oval stromal component
- focal old hemorrhage (not shown)
- intricate arrangement of stromal and glandular component.
Diagnosis: Extra-ovarian endometriosis
Discussion: Endometriosis is defined by the extra uterine presence of endometrial tissue. The ovary and fallopian tube along with the broad ligament are the most common sites of involvement. The large bowel and rectum are involved in approximately 15-20% of cases It is uncommon for peritoneal endometriosis to form a clinically significant mass lesion. Rarely, large endometriotic foci in the peritoneum measuring upto 15 cm and simulating a malignancy have been reported.
Complications of extraovarian endometriosis include rupture and/or hemorrhage of the endometriotic focus, yielding symptoms of an acute abdomen. Additionally, carcinoma arising in endometriosis is a well-documented complication of endometriosis irrespective of endometrial implant location. Endometrioid adenocarcinomas occur most commonly, followed by clear cell adenocarcinoma, and, rarely malignant mesodermal mixed tumors (MMMT) and endometrial stromal sarcomas.
Endometriotic foci are infrequently aspirated and thus may pose a diagnostic pitfall to the unsuspecting cytopathologist, particularly when the pertinent history of endometriosis is unavailable at the time of the fine needle aspiration. The key feature to evaluate and search for in cytologic preparations of endometriosis is the biphasic nature of the specimen: the glandular component intimately associated with the spindled stromal component. Foci of old hemorrhage and hemosiderin-laden macrophages may also be appreciated. These cytologic features recapitulate those seen in histologic sections of endometriosis. Fine needle aspiration of endometriosis may pose a sampling issue. In such cases, a conservative approach for the cytopathologist is best. A comment addressing the adequacy of sampling as well as the possibility of an unsampled malignancy, be it glandular, stromal or both, may be warranted with the added recommendation for complete excision if clinical concern for malignancy is high.
References:
Simsir, A, K Thorner, J Waisman, and J Cangiarella. Endometriosis in Abdominal Scars: A Report of Three Cases Diagnosed by Fine-Needle Apsiration Biopsy. Am Surg Oct 2001, 67(10): 984-988.
Kurman, R. Blaustein’s Pathology of the Female Genital Tract. 2002, 5 th ed.; 745-768.
Acknowledgement: This case is contributed by Lori Proctor, M.D. and Sanjay Logani, M.D. from the Department of Pathology, Emory University , Atlanta GA