Case of the Month ...
Case History
A 43 year old woman with a history of ovarian cancer presented for an annual screening mammogram. The mammogram demonstrated two new lesions: an indeterminate mass in the right breast at 11 o'clock, and another indeterminate mass in the left breast at 1 o'clock. A previous mammogram performed one year ago was unremarkable. On ultrasound, these masses were irregular, hyperechoic and vascularized, measuring 0.7 cm in the right breast, and 0.6 cm in the left. Both seemed to be located in the subcutaneous fat. The ultrasound findings were suspicious for metastatic carcinoma. An ultrasound guided fine needle aspiration biopsy (FNA) of both lesions, followed by a core biopsy of the left breast lesion, were performed.
Diagnosis & Discussion
click on image for larger version
Image Figs:
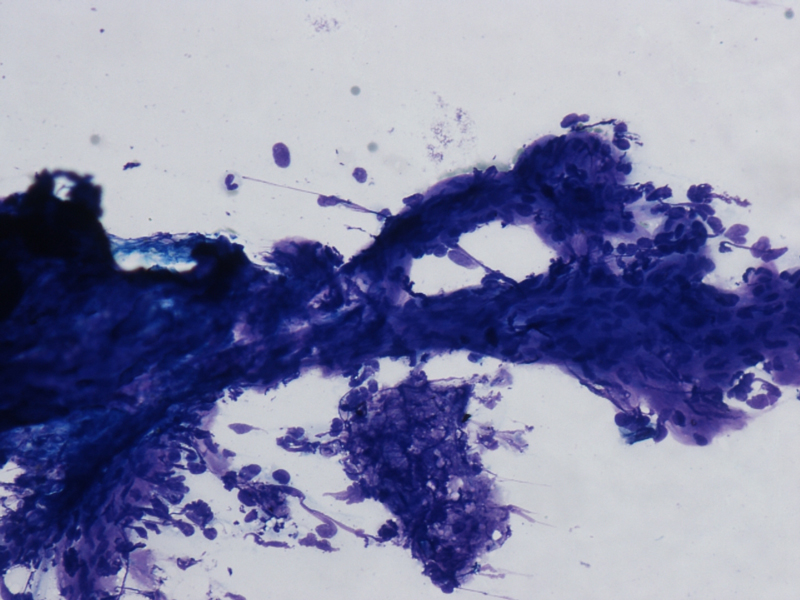
- FNA cytology smear of the left breast mass, Diff-Quik stain, x20
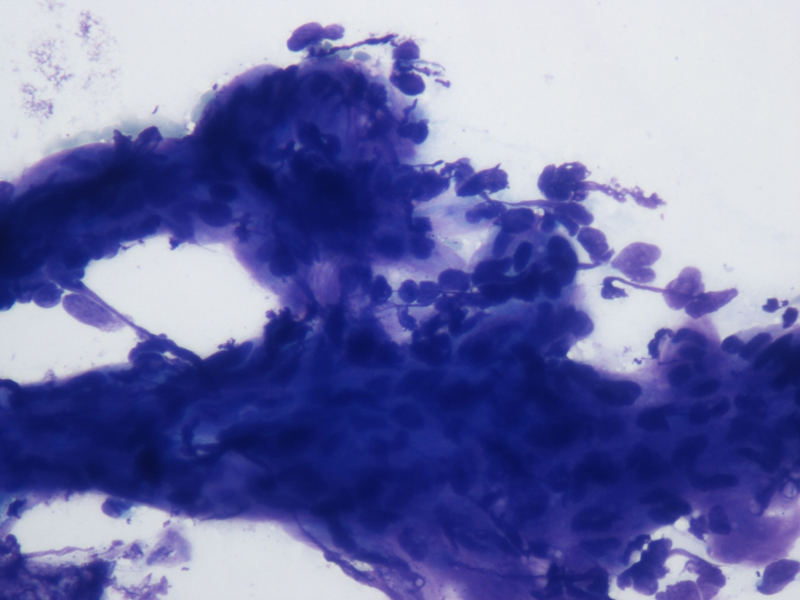
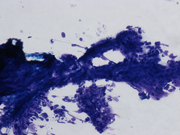
- FNA cytology smear of the left breast mass, Diff-Quik stain, x40
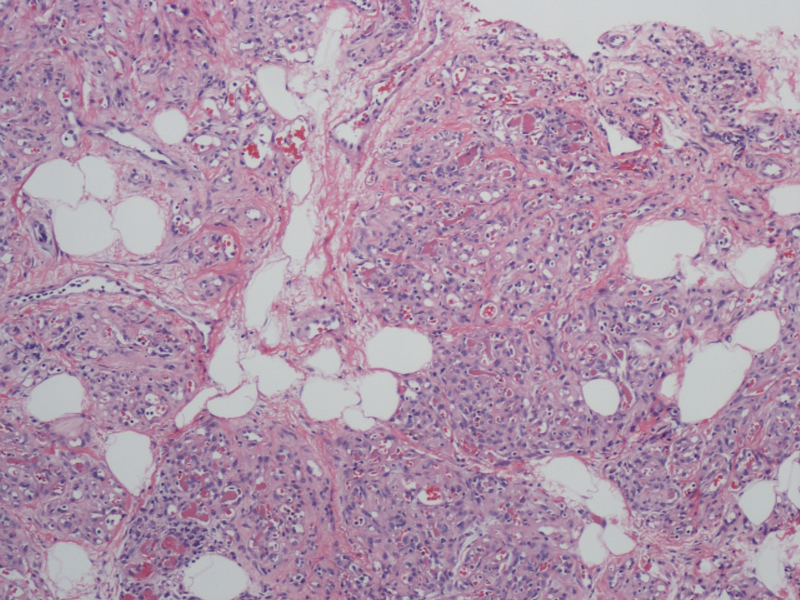
- Core biopsy of the left breast mass, H&E, x10
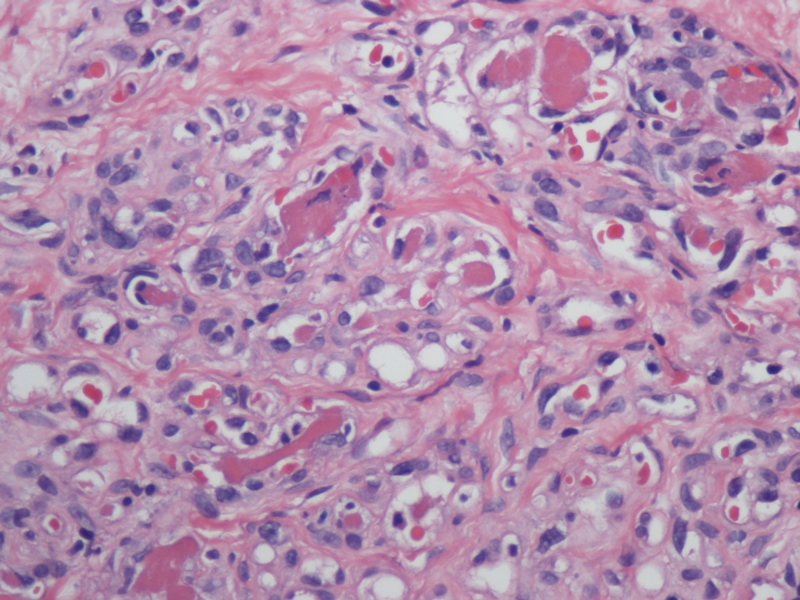
- Core biopsy of the left breast mass, H&E, x40
Questions:
What is the most likely cytologic diagnosis?
- Lipoma
- Angiosarcoma
- Hemangioma
- Angiolipoma
- Phyllodes tumor
- Which of the following lesions of the breast may demonstrate infiltrative borders?
- Angiolipoma
- Angiosarcoma
- Fibromatosis
- Radial scar
- All of the above
- A characteristic morphologic feature of this lesion is:
- Predominance of adipose tissue
- Fibrin thrombi
- Hobnailing endothelial cells
- Frequent mitotic figures
- These lesions in the breast are most frequently found in
- Subareolar area
- Adjacent to the chest wall
- Subcutaneous tissue
- Deep breast tissue
Discussion:
FNA smears were bloody and hypoecellular. They showed clusters of bland appearing spindled cell admixed with metachromatic matrix material, small vessels, and interspersed fat cells. The spindled cells were without significant nuclear atypia. No mitotic figures were noted. No mammary epithelial cells were seen. Based on the on site assessment diagnosis of spindle cell lesion, a core biopsy was performed. The core biopsy showed a proliferation of small capillary caliber vessels filled with blood with interspersed areas of adipose tissue. Fibrin thrombi were present in many of the capillary channels. No cytological atypia or mitotic figures were seen. CD34 immunostain confirmed the endothelial origin of the proliferating spindled cells. Ki67 index was below 5%, and HHV8 stain was negative. A diagnosis of angiolioma was made.
Angiolipoma is a benign tumor first described by Howard and Helwig in 1960. While not uncommon in the soft tissues of the trunk and upper extremities in young adults, angiolipoma is a rare lesion in the breast. It may be seen as a solitary mass or may present as multiple lesions. The age range is wide. The typical symptoms frequently associated with angiolipoma in various sites are pain and tenderness. When it occurs in the breast, angiolipoma is usually painless. Most breast angiolipomas are located relatively superficially in the subcutaneous tissue and measure less than 2 cm. Mammary angiolipoma does not have a typical mammographic appearance, and can be confused with malignant lesions. On ultrasound evaluation, angiolipoma presents as a hyperechoic mass, which is a relatively non-specific finding. If correctly diagnosed on FNA or core biopsy as angiolipoma, excision is not necessary as there is no malignant transformation.
Cytomorphology of angiolipoma is often described as strands of tightly packed small vessels and fat tissue fragments. Aspiration smears are usually hypocellular and contain predominantly mature adipose tissue with rare benign-appearing spindle-shaped endothelial cells arranged in clusters or strands, resembling capillaries. The smear background is hemorrhagic. Fibrin thrombi and mast cells may be seen. Histologically, mature adipose tissue is intimately intermixed with capilary-sized interanastomosing vascular channels. Adipose tissue and vessels together form a mass. Vascularity and cellularity vary from minimal to rich. Fibrin thrombi are present in almost all cases. Endothelial cells are usually bland and single layered without tufting, and/or papillary proliferation. Mitotic figures are absent in most cases. In the late stages, perivascular and interstitial fibrosis is noted. Two types of angiolipomas have been described: non-infiltrating and infiltrating. Most reported breast angiolipomas are non-infiltrating/well demarcated. Both types are benign.
Cytologic differential diagnosis of angiolipoma is broad and includes lipoma, hemangioma, Kaposi's sarcoma, angiosarcoma, fibroepithelial lesions in which the epithelial component is not well sampled among other less common spindled cell lesions. A specific diagnosis of angiolipoma in most cases is not possible by FNA due to overlapping features. Core biopsy diagnosis may also be problematic; lesions with low vascularity may be confused with adipose tissue and lipoma, and lesions with high vascularity and cellularity may cause concern for angiosarcoma. Presence of fibrin thrombi, the uniformly capillary nature of the vascular proliferation, and the absence of glandular breast tissue within the lesion are helpful in making a correct diagnosis of angiolipoma on core biopsy. However, excision may be necessary in some cases.
Answers
- d
- e
- b
- c
REFERENCES
Howard W, Helwig E. Angiolipoma. Arch Dermatol 1960; 82:924-31
Weinstein S, Conant E, Asc G. Angiolipoma of the breast. Radiology 2003; 227:773-5
Kryvenko ON , Chitale DA , VanEgmond EM , Gupta NS , Schultz D , Lee MW . Angiolipoma of the female breast: clinicomorphological correlation of 52 cases. Int J Surg Pathol. 2011 Feb;19(1):35-43
Weiss S, Goldblum J, Folpe A. Soft tissue tumors. 5 th edition. Mosby, 2007
Chhieng D, Cangiarella J, Waisman J. et al. Fine needle aspiration cytology of spindle cell lesions of the breast. Cancer 1999; 87(6):359-71
Ali S, Parwani A. Breast Cytopathology. Springer, 2007
Case contributed by
Alexander Finkelstein, MD and Aylin Simsir, MD
NYU School of Medicine
Department of Pathology
New York, NY